Disclaimer
• Your life and health are your own responsibility.
• Your decisions to act (or not act) based on information or advice anyone provides you—including me—are your own responsibility.
I’ve been working on several projects during the weeks I haven’t updated, and here’s the first. Epipheo—the people who make all those 3-minute cartoon visualizations of interesting ideas—contacted me some time ago, and asked if I was willing to help them create one based on an article of mine.
Usually when someone offers you something for “free”, they’re trying to sell you a timeshare. However, after a couple long recording sessions, some script wrangling, and several weeks, they’ve just sent me a link to their newest video visualization—based in part on my classic article “Why You’re Addicted To Bread”, and featuring narration by me!
It’s intended for a general audience, so it’s a bit of an oversimplification—but it’s a great start for when your Uncle Ned asks you “So why won’t you eat bread anymore?” So I encourage my readers to visit the Youtube page, drop a “Like” and/or a favorable comment, and spread it amongst your bread-eating friends. (Hint: share it on Facebook using the widget below.)
Bonus Video: Nose To Tail Eating With Big Primal and Primal North
A feast of heart, liver, sweetbreads, marrow, and more ‘odd bits’ from Big Primal—and some product placement, courtesy of Danny Albers from Primal North. (Youtube link.)
I recently visited the dentist for my regular six-month cleaning and checkup.
One mysterious practice you might recall from your own checkup is your hygenist probing around your gums with a pick, while calling out a bunch of numbers that someone else dutifully records in a computer.
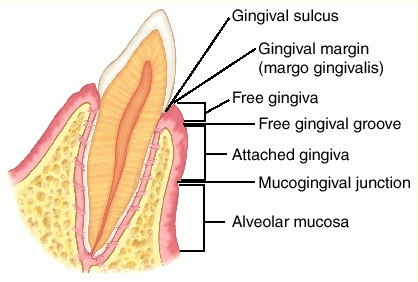
This isn’t some mysterious rite of Dental Magick: they’re measuring the depth of each gingival sulcus—the space between your tooth and your gums. Ideally, in a healthy mouth with healthy gums, this space is approximately 2mm deep, a depth easily reachable and cleanable by regular brushing.
However, most people do not have a healthy mouth with healthy gums. Somewhere between 30 and 50% of the US population has mild periodontitis (inflammation of the gums), with approximately 10% having severe periodontitis.
Plaque and Periodontitis: A Vicious Cycle
The usual cause of periodontitis is dental plaque (a bacterial biofilm), which accumulates in the gingival sulcus. The resulting inflammation causes the sulcus to deepen, beginning a vicious cycle: more plaque = more inflammation = deeper gingival sulcus = more plaque.
A depth of 4mm or more almost always indicates a degree of permanent damage and chronic infection, and is termed a periodontal pocket. Since pockets deeper than 3mm are generally too deep to clean by brushing one’s teeth at home, they tend to become deeper and worse over time, leading to chronic periodontitis—and a depth of 7mm creates a strong risk of tooth loss.
Even if the pockets never reach this depth, the continual low-grade oral infection of periodontitis (known colloquially as “gum disease”) causes systemic inflammation. We know this is a causal relationship, not just a correlation, because successful treatment of patients with severe periodontitis results in lower CRP and IL-6 levels:
Given this, the strong association of periodontitis (“gum disease”) with deaths from coronary heart disease (= CHD, = “atherosclerosis”, = the blockage of the coronary arteries due to arterial plaque) should not be surprising.
RESULTS: Periodontal disease with elevated markers of systemic bacterial exposure was associated strongly with CHD compared to subjects without PD, with a summary odds ratio of 1.75 (95% confidence interval (CI): 1.32 to 2.34; P <0.001). This group was not associated with CVD events or with stroke but was associated with a significant increase in mean CIMT (0.03 mm; 95% CI: 0.02 to 0.04).
In further support, periodontitis is associated with lower HDL, higher LDL, and increased non-fasting blood glucose:
Dental plaque is a bacterial biofilm that accumulates on our teeth.
Plaque causes tooth decay—because of the acids the plaque bacteria produce when they ferment sugars in our mouth.
A gingival sulcus (the space between tooth and gum) deeper than 3mm allows plaque to accumulate unmolested by regular brushing. Its ideal depth is 2mm.
Plaque accumulation is usually a vicious cycle: more plaque = more inflammation = deeper gingival sulcus = more plaque.
A sufficiently deep sulcus is known as a periodontal pocket, which usually leads to periodontitis (“gum disease”), and sometimes tooth loss.
Periodontitis causes systemic inflammation. It is associated with increased risk of heart disease, and with several bad metabolic markers.
Result: we would like all the measurements our dental hygenist calls out to be 2s (signifying a depth of 2mm), with perhaps a few 3s.
A Paleo Diet And My Own Gum Health: Some N=1 Data
I’ve cautioned about extrapolating based on personal experience (“N=1”) before, so I’ll preface this with “correlation is not causation, etc.” However, my warning applies primarily to proving the negative: just because something doesn’t make us feel bad or kill us within a few months doesn’t mean it’s either harmless or good for us!
If we take objective measurements and/or a consistent record of our observations, though, and are careful to evaluate possible confounders (was it that I started eating liver and pastured eggs, or that I got a new job and am sleeping better now that I don’t have to worry about making rent?), it’s often reasonable to correlate improvements with changes we’ve made.
To that end, here is some fascinating data I was able to obtain from my dentist’s office. I think the data is reasonably solid: my measurements were all taken by the same hygienist in the same office, I’ve used the same Sonicare toothbrush and kept the same program of indifferent dental hygiene, and my diet hasn’t changed radically.
Also note that I was already eating a strongly anti-inflammatory diet previous to “going Paleo”: I had independently found the original research on n-3/n-6 ratio, and had long since removed all seed oils from my diet (I was rendering my own beef tallow back in 2007!) The major dietary changes were going gluten-free, grain-free, and legume-free (except for occasional white rice), and dramatically decreasing my carbohydrate intake—mostly as a consequence of no longer eating bread or pasta.
I went Paleo between the first and second measurements. Therefore, the first set of measurements (#1 on the far left) is my pre-Paleo baseline.
Each tooth is measured six times: at the center and each edge, both front and back. Thus, there are 28x2x3 = 168 such measurements if your wisdom teeth have been removed, 192 if you still have them. For those interested in the raw data, here’s a scan:
Note that there are no 4mm pockets at all after the third set of measurements.
Result: starting from a reasonably healthy mouth and an already strongly anti-inflammatory baseline diet, my oral health has improved dramatically—to the point that my dentist told me “Your teeth are great! Whatever you’re doing, keep doing it.”
I have also experienced subjective improvements. My teeth are much less sensitive than before: I used to dread the approach of the electric tooth scaler at each cleaning (it was painful to the point that I would white-knuckle the armrests) but now it doesn’t bother me at all. They’re far less sensitive to cold as well, and less prone to bleeding when I neglect to floss for days or weeks.
In short, while I can’t rule out coincidence, it certainly appears that my excellent dental health is strongly correlated with eating like a predator.
Different schools of nutrition argue endlessly about protein. Vegans swear it destroys our kidneys and we’re eating far too much. Strength athletes and leangains devotees can’t get enough. The government claims 56 grams/day is more than enough for anyone—yet even the most conservative and fat-friendly paleo templates recommend closer to 90 grams. Paleo eaters and omnivores enjoy pointing out that animal protein is “complete”, unlike most grain and vegetable proteins, while vegetarians and vegans swear by “protein combining”. And just about everyone gets confused when acronyms like BV, NPU, and PDCAAS enter the picture.
What Is Protein, Anyway?
Talking about “protein” is like talking about “buildings”. Just as “building” can mean a single-family home, a chemical factory, a mud-and-straw hut, a skyscraper, or the Taj Mahal, “protein” can mean anything from tiny di- and tri-peptides containing perhaps a few dozen atoms, to the giant linked chains of keratin that make up our hair and fingernails.
As such, it turns out that “protein” is a term so broad as to be nearly useless when applied to nutrition. When we’re asking the question “How much protein should we eat?” what we’re really asking is “Which amino acids do we require, what relative proportions to we require them in, and to what degree are the foods containing them digestible, bioavailable, and not otherwise poisonous or disruptive to our metabolism when ingested?”
If that sentence wasn’t immediately comprehensible to you, fear not—the purpose of this article is to explain it!
What is Protein Made Of?
Proteins are molecules made up of amino acids stuck together by peptide bonds.
Amino acids are so named because they contain both an amine group (-NH2) and a carboxyl group (-COOH). In the renderings below, we can see the carboxyl groups (the two red balls with one white ball attached) and the amine groups (the blue ball with two white balls attached). The alpha carbon, to which they’re both attached, is colored black. Here are a few examples:
Lysine
Tyrosine
Valine
Cysteine
Click here to see the 2D and 3D structure of all 21 standard amino acids.
A peptide bond occurs when the carboxyl from one amino acid bonds covalently to the amine of another—releasing a molecule of water in the process. Result: we can make just about any shape and size of protein we want by stringing together the right amino acids in a single-file chain, carboxyl to amine.
Strictly speaking, all the biologically important amino acids are alpha-amino acids, in which the amine and the carboxyl are both attached to the first carbon atom. The term “amino acid” usually refers only to the alpha-amino acids.
What Can Proteins Do?
It turns out that proteins are extremely versatile molecules. They are the basic machinery of all cells: DNA is, quite literally, just instructions for building proteins out of amino acids. They catalyze chemical reactions (“enzymes”), they signal metabolic and immune events (e.g. insulin, leptin, growth hormone, antibodies), they transport oxygen (hemoglobin and myoglobin), and they’re structural components of everything from the cytoskeleton and mitochondria of every cell to our tendons, ligaments, hair, nails, and connective tissue. Even the parts of a cell which are made from other molecules, such as phospholipids and polysaccharides, are ‘built’ by their interaction with proteins!
The average human cell is approximately 65% water, 20% protein, 12% lipid (fat), 1% RNA and DNA, and 2% “other” by mass. (Freitas 1998)
Why Do We Need To Eat Protein?
Of the 21 amino acids coded for by the DNA of multicellular organisms, adult humans can only synthesize 12 of them. The other nine must be consumed in the diet, so we call them essential amino acids.
It’s actually far more complicated than “essential” or “non-essential”. Some amino acids can be converted to each other, but not created from scratch. Some amino acids can be synthesized, but not rapidly enough to meet all our metabolic needs. And children can’t synthesize some of the amino acids that adults can.
Result: humans have a non-negotiable requirement for dietary amino acids in order to sustain the basic processes of life.
Why Do We Need To Eat Protein Every Day?
Some nutrients, like vitamin B12, are stored within the body and released when needed—so though we must consume a certain amount on average, we don’t have to do so every day in order to keep ourselves healthy.
Unfortunately, we have no way to store amino acids. We have a tremendous capacity to store fat in fat cells, and a very limited capacity to store glucose (as glycogen in our muscles and liver)—but we must either use amino acids to synthesize proteins, burn them for energy, convert them to glucose, or (very rarely, and if all else fails) excrete them.
Therefore, humans have a daily requirement for each one of the amino acids necessary to life, in the quantities required by whatever proteins the trillions of cells in our bodies are making (minus our ability to synthesize some of them).
Why “Complete Protein” Is Important
Imagine a factory that assembles cars. Let’s say you have 400 wheels and tires in inventory, 200 headlights, 100 chassis, 100 engines…but only ten steering wheels. It doesn’t matter that you’ve got almost enough parts to build 100 cars: ten steering wheels means you can build ten cars. Whichever part you have the fewest of limits how many cars you can build.
Our bodies have the same problem when building proteins. For instance, lysine is an essential amino acid—so if we haven’t consumed any lysine, we can’t build any proteins that contain lysine, no matter how many of the other amino acids are available. This leaves us with two options:
Don’t build that protein. This is not usually a viable option, as it results in signals not reaching the intended recipient, damaged cells and tissues not being repaired, pathogens not being attacked…in other words, the failure of basic metabolic processes.
Disassemble existing tissues in order to get the amino acid(s) we need. This is known as catabolysis or ‘going catabolic’, and is what actually occurs. Muscles are the first tissues to be catabolized, as becoming slightly weaker is usually less harmful than impairing the function of other organs.
Our Summary (so far)
Proteins form the basic machinery of all cells.
Proteins are made out of amino acids.
Amino acids are not interchangeable: to synthesize a protein, each one of its constituent amino acids must be available.
Many amino acids are essential—we cannot synthesize them, and therefore must ingest them as part of our diet. Many others are conditionally essential, and cannot be synthesized or converted at the rate we require them.
Since we have no way to store amino acids for later use, our bodies have a daily requirement for them.
Therefore, we must ingest each amino acid, roughly in the proportion we require it, every day.
Conclusion
Our biological needs are for specific amino acids in specific proportions, but “protein” can mean any combination of one or more amino acids. Therefore, the amount of “protein” in food is, by itself, a nearly meaningless number.
I’ll discuss measures of protein quality, and much more, next week!
Live in freedom, live in beauty.
JS
Do you find this article helpful? Share it using the widget below! Got questions? Leave a comment.
Support gnolls.org by making your Amazon.com purchases through this affiliate link:
It costs you nothing, and I get a small spiff. Thanks! -JS
.
Subscribe to Posts
Gnolls In Your Inbox!
Sign up for the sporadic yet informative gnolls.org newsletter. Since I don't update every day, this is a great way to keep abreast of important content. (Your email will not be sold or shared.)
IMPORTANT! If you do not receive a confirmation email, check your spam folder.